Acute coronary syndromes algorithm: Assessments and actions
 Written by Judy Haluka
Written by Judy Haluka
Changes: AHA 2025 updates - medical writer text revisions
In the presence of ACS, EMS or the Emergency Department will start with care and focus on obtaining a 12-lead ECG, aspirin administration, oxygen therapy if oxygen saturation is <90% or if the patient is short of breath, administering nitroglycerin if not contraindicated and/or morphine/fentanyl for discomfort if no relief with nitroglycerin, and most importantly activating the cardiac cath lab. In the initial minutes of care, the patient will have vital signs obtained, IV access established, and a physical examination performed. The ED/cath lab team will obtain cardiac markers, CBC, and coagulation studies. A chest x-ray should also be completed. The ED/cath lab will also consider P2Y12 inhibitors as an adjunct therapy.
Printed crash cart cards

Order the full set of printed crash cart cards.
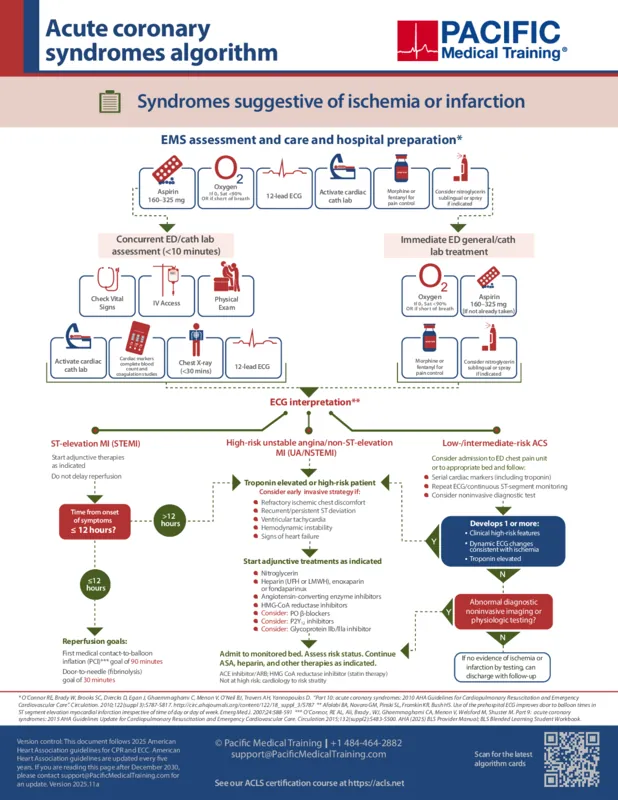
If the patient is having an ST-elevation MI (STEMI), adjunctive therapies must be started immediately with the goal of reperfusion as soon as possible. If the STEMI has evolved in less than 12 hours, the goal from first medical contact to the balloon inflation (FMC-to-balloon) is 90 minutes. The goal of door-to-needle (fibrinolysis) is 30 minutes. Meaning, the time from when the patient got to the ER to the time of fibrinolysis should be less than 30 minutes.
If the time of onset of symptoms is more than 12 hours, the patient has high-risk unstable angina, has non-ST elevation MI, has refractory ischemic chest discomfort, recurrent or persistent ST deviation, ventricular tachycardia, hemodynamic instability, or signs of heart failure, start Adjunct treatments include nitroglycerin, heparin (UFH or LMWH), enoxaparin or fondaparinux, angiotensin-converting enzyme inhibitors, HMG-CoA reductase inhibitors, oral beta blockers, P2Y12 inhibitors, and glycoprotein IIb/IIIa inhibitors. This patient should be admitted to a monitored bed and continued on therapies as indicated.
A patient with low/intermediate risk for acute coronary syndrome should have cardiac markers, CBC, and coagulation studies. They should have repeated ECG and continuous ST-segment monitoring and should consider non-invasive diagnostic tests. If they develop any high-risk features, ECG changes, or elevated troponin levels, treat them as high-risk ACS patients. Also, if they have abnormal noninvasive imaging or physiologic testing, they should be treated as high-risk ACS patients. If there is no evidence of ischemia or infarction by testing, the patient can follow up with their primary care doctor or cardiologist.

Planning to certify/recertify ACLS?
Get a reminder when you need to take the exam
Please verify or enter a different email address:
How we reviewed this article
Our experts continually monitor the medical science space, and we update our articles when new information becomes available.
- Current versionMail the author of this pageEmail
- Feb 19, 2026
Reviewed by:
Changes: AHA 2025 updates - medical writer text revisions- Jul 29, 2021
Written by:
