ACLS instruction videos
Also see these videos from our YouTube page
ACLS videos
Waveform capnography
A new tool for life support, waveform capnography allows you to assess the effectiveness of compressions and stability of the victim. This is effective for the perfusing patient and during cardiac arrest.
Intraosseous medication

Drills straight to the core of IO administration, shows the most common placement and how get medication access.
King airway usage

Introduction to and proper usage of King airway for advanced airway creation. Blocks air from escaping to esophagus or mouth and guides into lungs.
Basic life support videos
Heimlich maneuver

Basic demonstration of Heimlich maneuver technique and advanced demonstration of aiming technique.
Defibrillator & paddle usage

Shows how to use the defibrillator and different ways to place the paddles with discussion of how to choose.
CPR compression
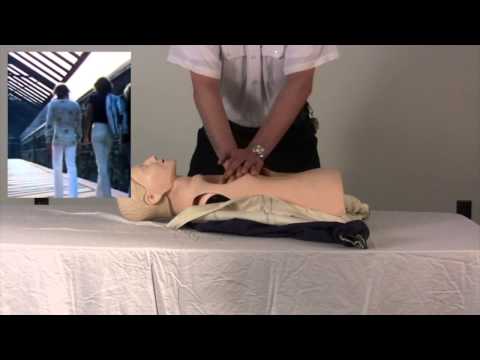
Demonstrates how to perform good chest compressions and tips to make it easy to remember.
Bag valve ventilation

Performing bag valve ventilation with one or two rescuers.
Basic life support with AED

Demonstrates chest compressions and air bag used with AED.
Arrhythmia interpretation / Monitor tech
Normal sinus rhythm
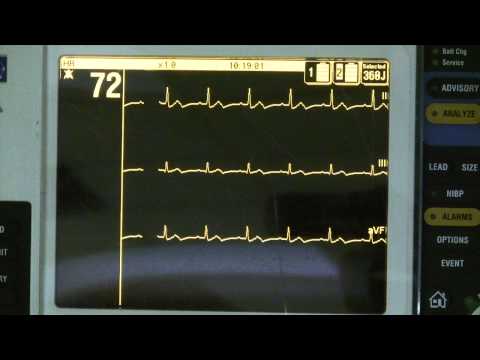
- Heart rate = 60–100 beats per minute
- Regular rhythm — slight irregularities are normal
- P waves precede each and every QRS complex
- The PR interval is between 0.10 and 0.20 seconds
- The QRS complex is within normal limits 0.08 – 0.12 seconds
- There is a QRS complex following each and every P wave
Asystole

Asystole — is the absence of electrical and mechanical activity in the heart. P waves may be present but there are either no QRS complexes or less than 15 QRS complexes per minute. This rhythm usually is an indication of death. This is the rhythm that is routinely referred to "flat line."
PSVT
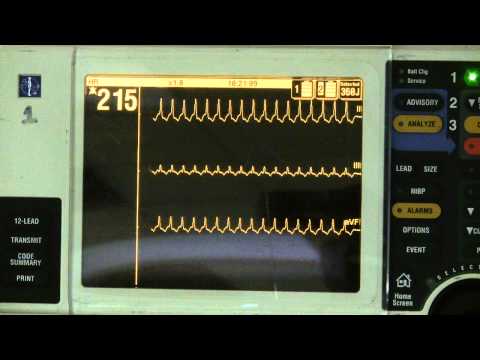
Is used to describe any rhythm that originates above the ventricles that is fast. The result is a fast narrow complex tachycardia. SVT is used when the rhythm is going so fast that it is impossible to distinguish P waves or PR intervals or even regularity of the strip.
Atrial fibrillation

Any rhythm that is grossly irregular and you cannot find P waves an accurate guess would be atrial fibrillation. A good way to tell the difference between atrial flutter and atrial fibrillation is that if you were asked to count the atrial rate it would be possible in atrial flutter because there are discernible flutter waves. It would not be possible to count an atrial rate in atrial fibrillation.
2nd degree AV block mobitz I
Second degree AV block Mobitz I (Wenckebach). The only difference in this ECG strip and that of sinus rhythm is that the PR interval is longer. This is because it is taking longer for the impulse to travel from the SA node to the ventricles to cause depolarization. This AV block is usually benign although in patient’s with heart disease it can signal that more advanced AV blocks may be just around the corner.
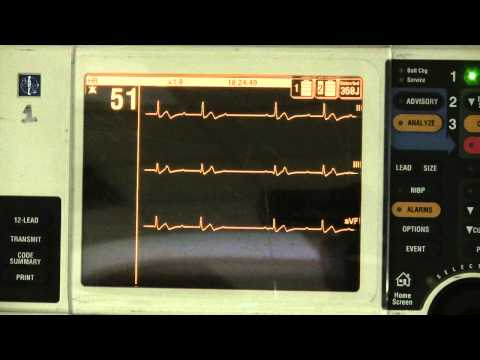
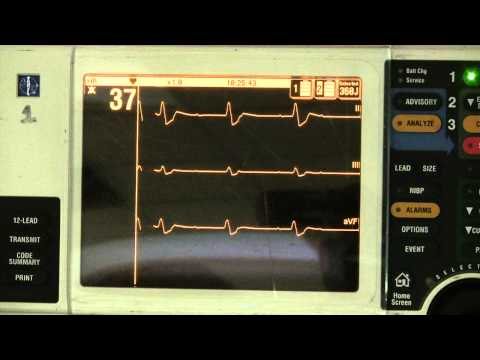
Sinus bradycardia
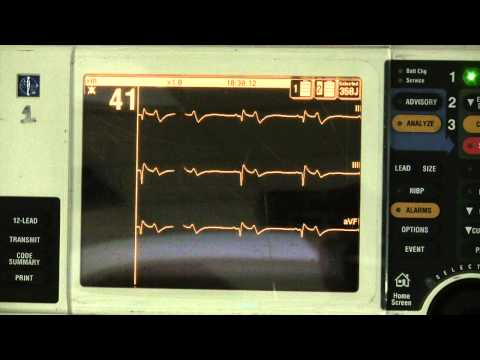
You will note that the only difference between normal sinus rhythm and sinus bradycardia is the heart rate. When you first learn how to interpret rhythms pay attention to the name (not the abbreviation) and it will give you a hint as to what it looks like. Rhythms are named first by the pacemaker site, then by the ectopic focus (if there is one) and then by the heart rate. For example, sinus bradycardia originates in the sinus node and the heart rate is less than 60 (bradycardia).
Sinus tachycardia
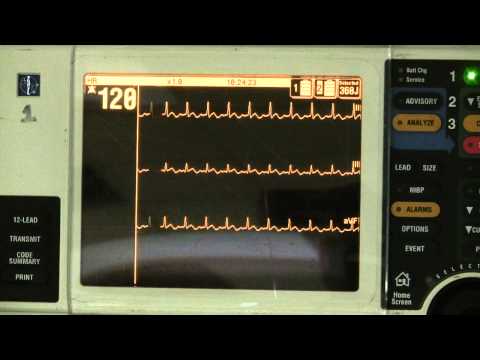
Sinus tachycardia originates in the sinus node and is faster than 100 beats per minute. Sinus tachycardia is always compensating for something. For example, if a patient is bleeding, the first thing the body will do is to increase the heart rate so that the blood that is left is pumped around faster.
Atrial flutter

Atrial flutter occurs when the atrium fires at such a fast rate that P waves become indiscernible. They instead blend together to become "flutter or F waves". In atrial flutter, the atria do not contract putting the patient at high risk to develop blood clots originating in the appendage of the atria.
Third degree heart block
Third degree heart block ("complete block") can be asymptomatic; however always requires the implantation of a permanent pacemaker because it represents complete failure of the AV node leaving only one very non efficient pacemaker left (the ventricles).
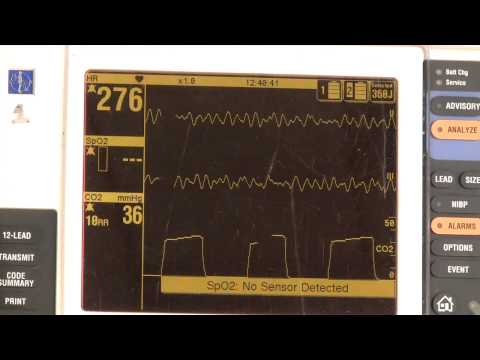
Torsades de pointes
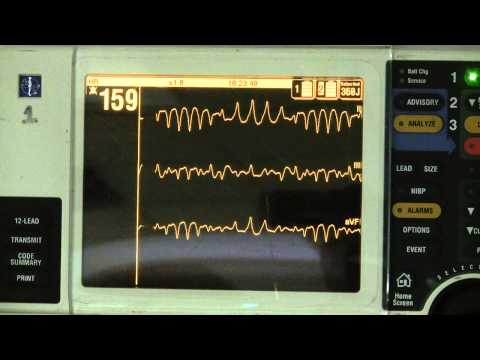
This is a polymorphic VT that has the distinct characteristic of QRS complex coming into and out of the isoelectric line. This can quickly degrade into VF leading to sudden death without intervention or revert to normal sinus rhythm.
Ventricular fibrillation
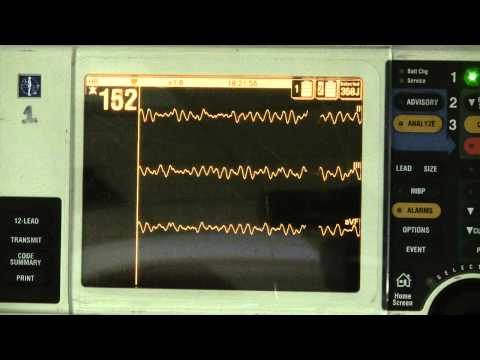
Ventricular fibrillation always represents a life threat. Hundreds or thousands of focuses are firing at the same time causing chaotic motion of the ventricle. If you were to look into the chest of a patient in ventricular fibrillation the heart would look as if you had jello placed in a bowl and then bumped the bowl.
Ventricular tachycardia
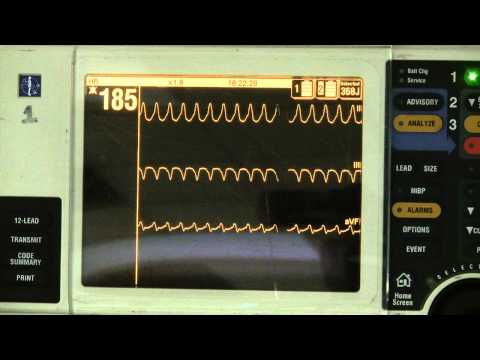
Because the rhythm is not efficient, and fast it rarely without symptoms. In fact, ventricular tachycardia can be a rhythm of cardiac arrest without pulses.
More free study resources
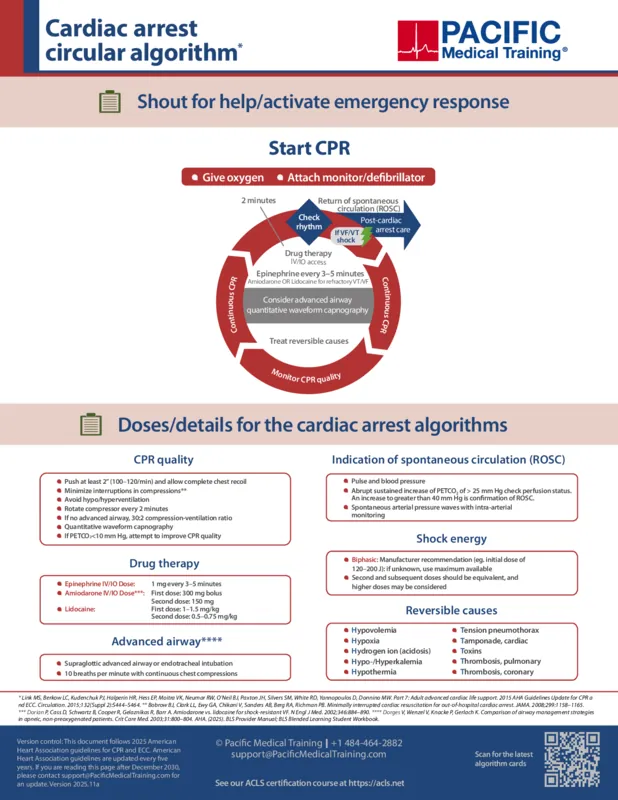
ACLS algorithms
A full showcase of the ACLS algorithms including diagrams for care of the megacode cases.Quizzes
Case-study based ACLS pretest review, brush up on skills from your RN courses with these free quizzes for cardiac diseases.
Planning to certify/recertify ACLS, BLS, or PALS?
Get a reminder when you need to take the exam
Please verify or enter a different email address:
How we reviewed this article
Our experts continually monitor the medical science space, and we update our articles when new information becomes available.
- Current versionMail the author of this pageEmail
- Jan 4, 2015
Written by:
Changes: Initial publication of ACLS instruction videos
