ACLS suspected stroke algorithm: Managing acute ischemic stroke
 Written by Judy Haluka
Written by Judy Haluka
Changes: Updated text for grammar and accuracy
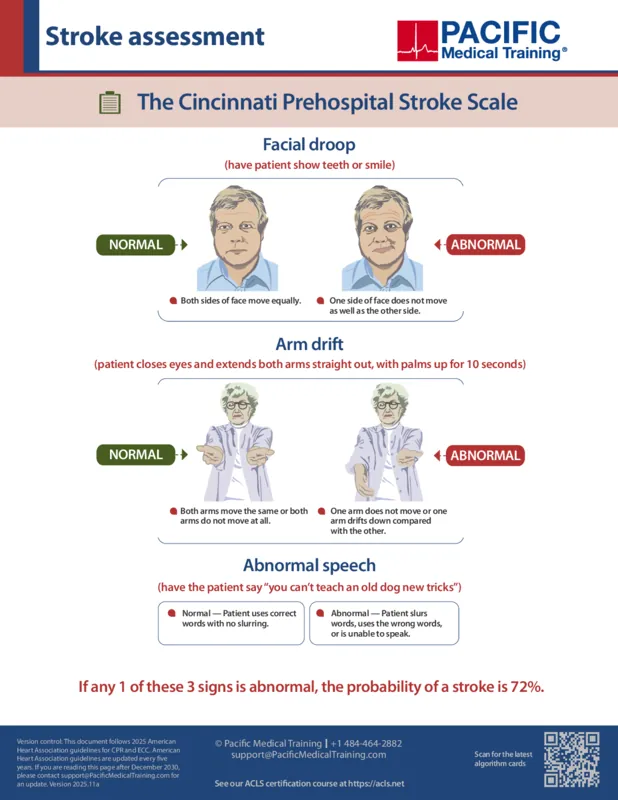
To test for stroke probability, instruct the patient to show their teeth or smile. Evaluate for facial droop. It is abnormal if one side of the face does not move as well as the other. Next, evaluate arm drift. Instruct the patient to close their eyes and extend both arms straight out, with the palms up, for 10 seconds. It is abnormal if one arm does not move or if one arm drifts down compared with the other. Third, evaluate for abnormal speech. Have the patient say, "You can't teach an old dog new tricks." It is abnormal if the patient slurs words, uses the wrong words, or is unable to speak. If any one of the 3 signs is abnormal, the probability of a stroke is 72%.
Printed crash cart cards

Order the full set of printed crash cart cards.
Identify signs and symptoms of a possible stroke and activate the emergency response system.
Pre-hospital interventions by EMS will focus on supporting ABCs and giving oxygen if indicated, performing a prehospital stroke assessment using an approved tool such as the Cincinnati Stroke Scale, checking glucose, establishing time of symptom onset (or last seen normal), triaging to a stroke center, and alerting the hospital to activate the stroke team.
Within 10 minutes of ED arrival, perform an immediate general assessment and stabilize the ABCs if necessary. Provide oxygen therapy if hypoxic. Obtain IV access and perform laboratory assessments.
Check glucose and treat if indicated. Obtain a 12-lead ECG and perform a neurologic screening assessment. Do not delay CT: obtain CT without contrast within 20 minutes of patient arrival.
A neurologic assessment by the stroke team or designee should be performed within 20 minutes of the patient's arrival to the ED. Review the patient's history, determine the time of symptom onset or the last known normal, and perform a neurological examination using a standardized tool such as the NIH Stroke Scale or the Canadian Neurological Scale.
If the CT scan shows hemorrhage, consult a neurologist or neurosurgeon and consider a transfer. Begin stroke or hemorrhage pathway. Admit to a stroke unit or intensive care.
If the CT scan shows no hemorrhage, consider fibrinolytic therapy. Check for fibrinolytic exclusions, and repeat the neurologic exam to determine whether symptoms are improving or worsening.
Candidates with the onset of symptoms within 3 hours or 4.5 hours in selected patients are eligible.
If the patient is a candidate for fibrinolytic therapy, review the risks and benefits with the patient and family. Begin fibrinolytic therapy within 60 minutes of patient arrival to the ED. Consider endovascular therapy for the onset of symptoms within 24 hours and for large-vessel occlusion. Admit the patient to stroke care within 3 hours of ED arrival.
Begin post-fibrinolytic stroke care. Monitor blood pressure and neurological symptoms. Monitor for adverse reactions to fibrinolytic therapy.

Planning to certify/recertify ACLS?
Get a reminder when you need to take the exam
Please verify or enter a different email address:
How we reviewed this article
Our experts continually monitor the medical science space, and we update our articles when new information becomes available.
- Current versionMail the author of this pageEmail
- Feb 19, 2026
Reviewed by:
Changes: Updated text for grammar and accuracy- Jul 26, 2021
Written by:
