ACLS algorithms for advanced cardiac life support
One of the crucial components of effective ACLS training is a familiarity with the major algorithms for different patient and/or provider scenarios. As a free resource for our visitors, this page contains links to sample algorithms for the main AHA advanced cardiac life support cases. See our website terms. Compatible part number: 90-1010.
See our separate pages for BLS algorithms and PALS algorithms.
 ACLS crash cart algorithm pocket cards.
ACLS crash cart algorithm pocket cards.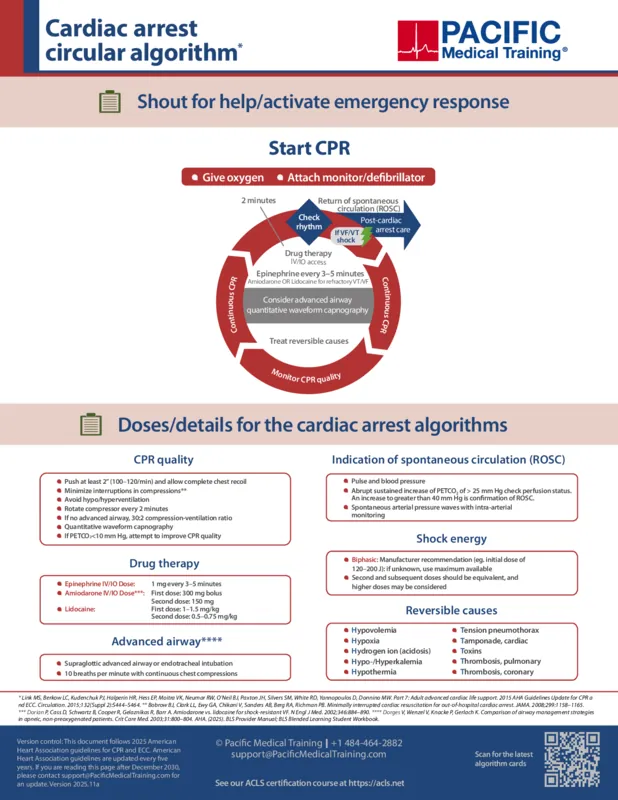
Cardiac arrest ACLS algorithm
This case presents the recommended assessment, intervention, and management options for a patient in respiratory arrest. The patient is unresponsive and unconscious. Respirations are absent or inadequate to maintain effective oxygenation and ventilation. The patient has a pulse. Even though the patient is in respiratory arrest and not in cardiac arrest, the BLS Primary Survey and the ACLS Secondary Survey are used.
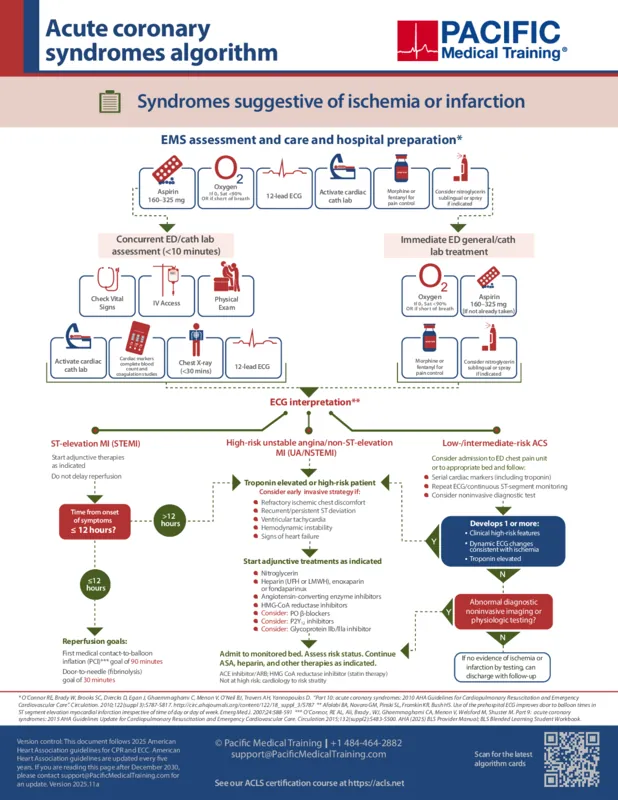
Acute coronary syndromes (ACS) algorithm
For this case, you use the acute coronary syndromes (ACS) algorithm to guide the assessment and management of patients with signs and symptoms of acute coronary syndromes. A key focus of the case is the identification and treatment of ST-segment elevation myocardial infarction (STEMI). You use a 12-lead ECG to evaluate the patient's rhythm. You initiate treatment based on your assessment.
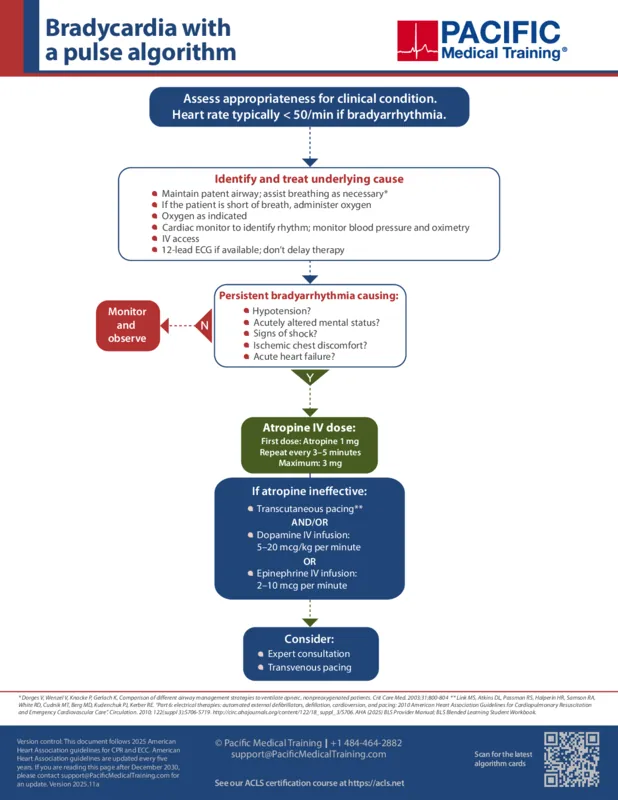
Bradycardia ACLS algorithm
This case outlines how to assess and manage a patient with symptomatic bradycardia. The patient has a pulse. One of your tasks is to figure out if the patient's signs and symptoms are caused by the slow heart rate or have an unrelated cause. Another task is to correctly diagnose the presence and type of atrioventricular (AV) block and implement the correct management strategies for AV blocks. You also need to know the techniques and cautions for using transcutaneous pacing.
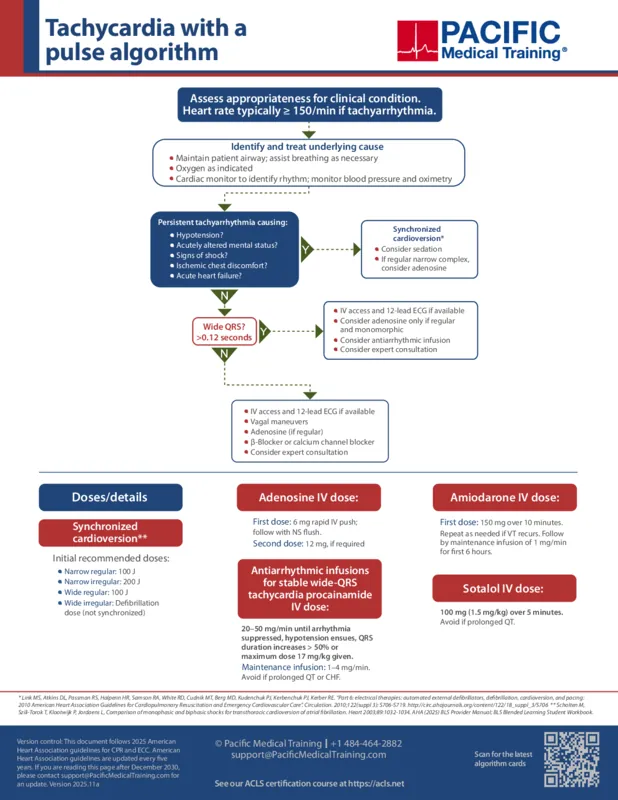
Tachycardia ACLS algorithms
This case presents the assessment and management of a stable patient with a pulse who has a heart rate greater than 100 bpm. Your tasks are to classify the tachycardia as narrow or wide, regular or irregular, and to implement the appropriate interventions from the ACLS Tachycardia Algorithm, including vagal maneuvers and adenosine. Monitor the patient's rhythm and request a cardiac consultation if the patient's rhythm does not convert. If the patient becomes unstable, follow the algorithm for unstable tachycardia. For unstable tachycardia, you evaluate the patient for cardioversion and perform the procedure. Drugs are not used to manage unstable tachycardia.
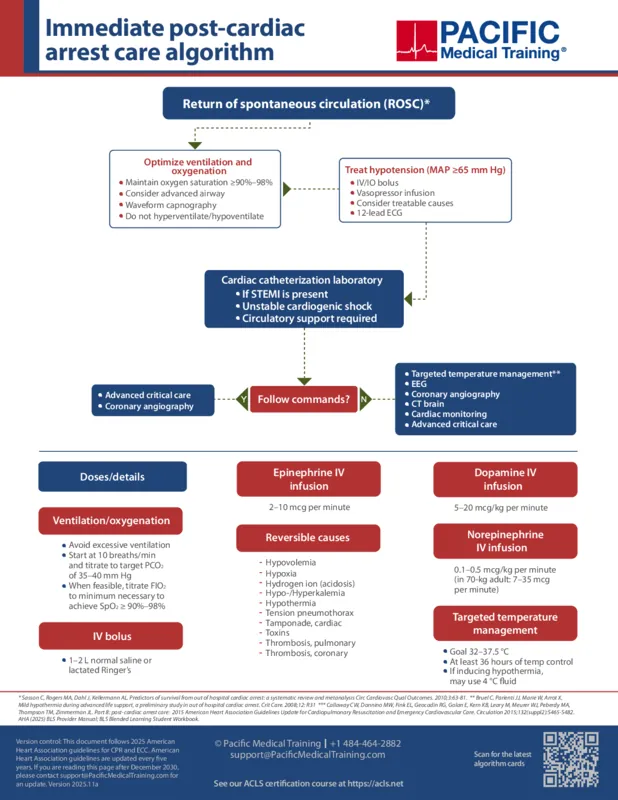
Post-cardiac arrest care ACLS algorithm
This case presents how to respond to someone who collapses outside of the hospital setting from either ventricular fibrillation (VF) or ventricular tachycardia (VT). You are alone and must manage the patient by yourself. You do not have the option of ACLS interventions which you learned from ACLS online certification, including advanced airway control and IV medications. You have an automated external defibrillator (AED) with a pocket face mask. The second AED case focuses on the assessment and management of a patient in a witnessed cardiac arrest caused by ventricular fibrillation (VF) or pulseless ventricular tachycardia (VT). The patient did not respond to the first shock. A manual defibrillator is used in this case, and you work with a care team.
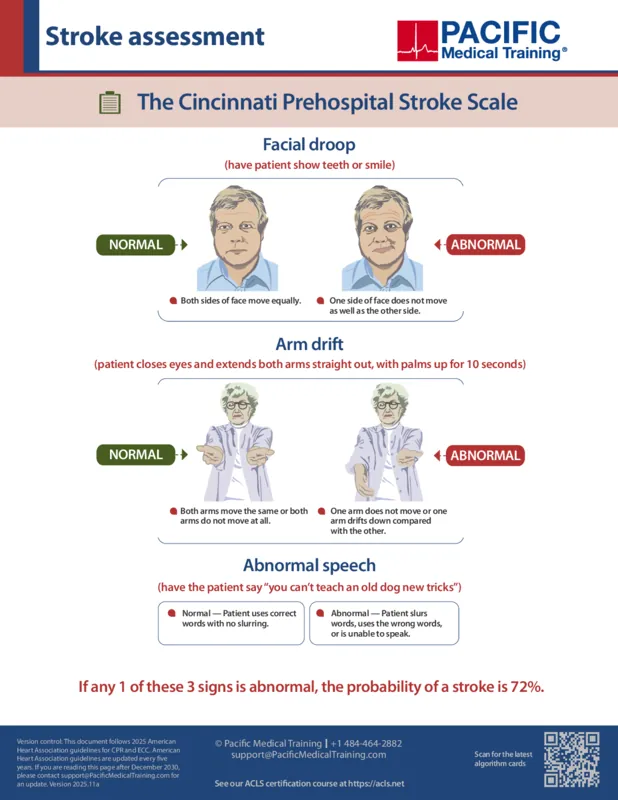
Suspected stroke ACLS algorithm
This case presents the identification (Cincinnati Prehospital Stroke Scale) and initial management of patients with acute ischemic stroke, a sudden change in neurological function brought on by a change in blood flow to the brain. This case is in scope for ACLS providers and covers fundamental out-of-hospital care, as well as basic aspects of initial in-hospital acute stroke care. This includes out-of-hospital and in-hospital situations, and National Institute of Neurological Disorders and Stroke (NINDS) time goals.
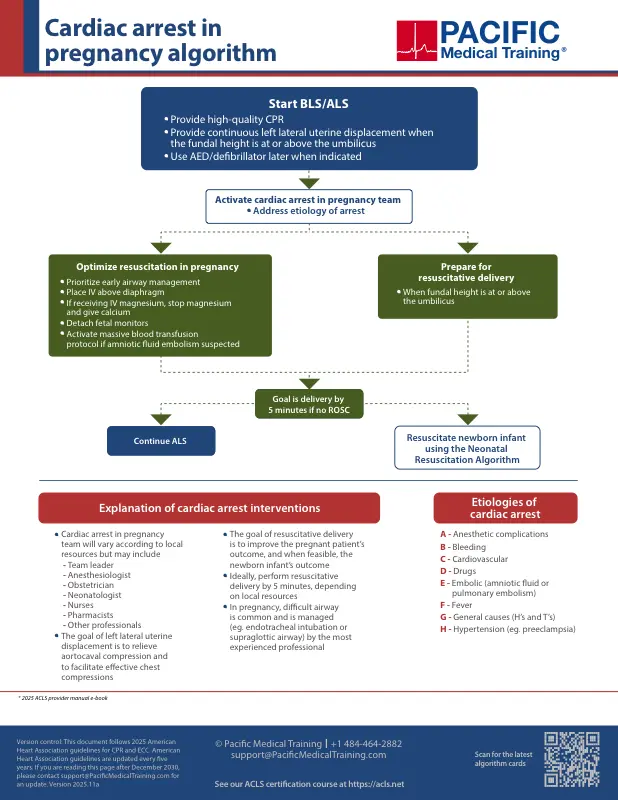
Cardiac arrest in pregnancy algorithm
This case presents how to manage cardiac arrest in pregnancy with modifications to optimize maternal and fetal outcomes. Key interventions include left lateral uterine displacement when fundal height is at or above the umbilicus, early airway management, IV access above the diaphragm, and preparation for resuscitative delivery within five minutes if no return of spontaneous circulation.
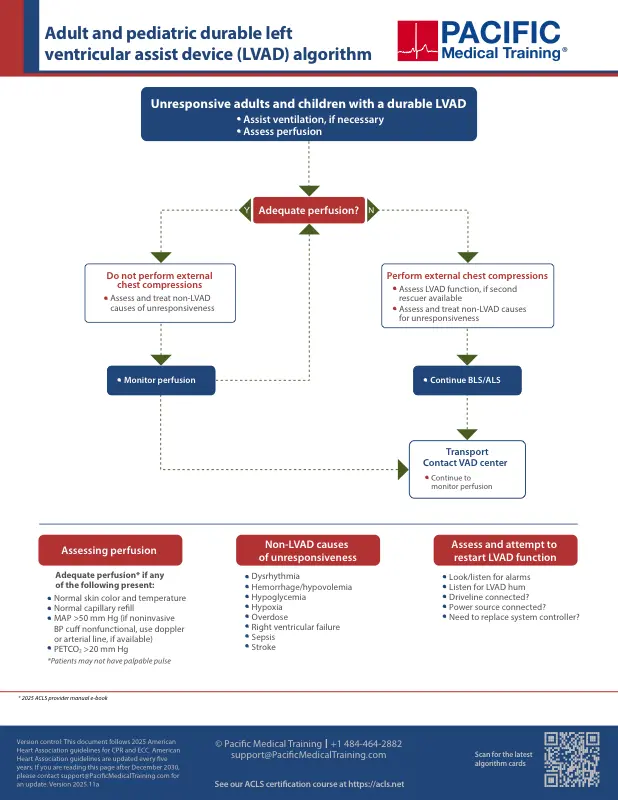
Durable LVAD algorithm
This case presents assessment and management of unresponsive patients with a durable left ventricular assist device (LVAD). Continuous-flow LVADs may produce little or no pulse, so assess for perfusion rather than relying on a palpable pulse. External compressions should only be initiated when perfusion is inadequate. Troubleshoot LVAD function and address reversible non-LVAD causes.


Other free study resources
Watch our ACLS instructional videos and prepare for renewal with our practice quizzes.

Planning to certify/recertify ACLS?
Get a reminder when you need to take the exam
Please verify or enter a different email address:
ACLS anesthesia algorithms
These algorithms involve ACLS events in in-hospital settings for anesthetic and surgically related pathophysiology. Thank you to Vivek K. Moitra, MD, Andrea Gabrielli, MD, Gerald A. Maccioli, MD, and Michael F. O’Connor for providing this to us. Printed with permission.
Vivek K. Moitra, MD, Andrea Gabrielli, MD, Gerald A. Maccioli, MD, and Michael F. O’Connor, MD. Can J Anaesth. 2012 June; 59(6): 586-603.

How we reviewed this article
Our experts continually monitor the medical science space, and we update our articles when new information becomes available.
- Current versionMail the author of this pageEmail
- Dec 3, 2025
Copy edited by:
Copy editorsChanges: Replaced algorithm images with 2025 AHA guidelines- Jul 1, 2021
Written by:
